
Transnasal endoscopic surgery in Pune, performed by Dr. Sarang Gotecha at Manipal Hospital, Baner, removes pituitary tumors through the nostrils - no skull incision, no visible scar. This approach treats functioning and non-functioning pituitary adenomas, with hospital discharge in 2–3 days and vision improvement measurable within weeks post-operatively.
Open with the disconnect between public perception and surgical reality: most people, when told they have a 'brain tumor,' assume they will need a visible scar, a shaved head and months of recovery. For pituitary tumors - among the most common type of brain tumor, accounting for 10–15% of all primary brain tumors - this is completely avoidable. Transnasal endoscopic surgery reaches the pituitary gland through the nostrils, leaving no external sign that surgery has occurred. This is not experimental - it has been the standard of care at major centres globally since the late 1990s.
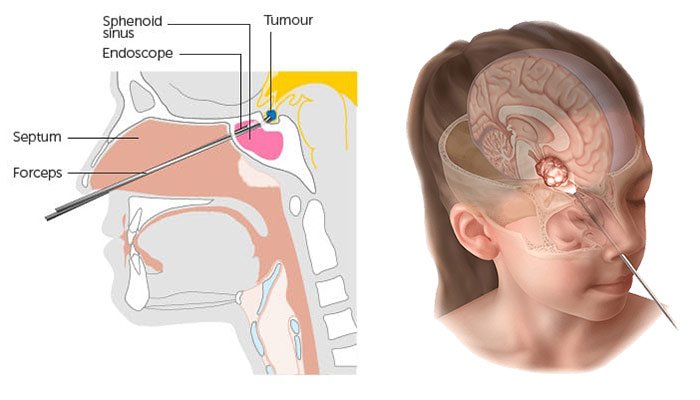
The idea of accessing the brain through the nose sounds counterintuitive - but it is, for pituitary tumors, the most direct route available. The pituitary gland sits in a bony saddle (the sella turcica) at the base of the skull, directly behind the nasal passages. Working through the nasal cavity and the sphenoid sinus, a surgeon can reach this gland and the tumors growing on it without making a single incision on the scalp or the outside of the skull.

This approach - the endoscopic endonasal (through-the-nose) transsphenoidal route - has replaced the older microscopic approach at most major neurosurgical centres globally. The field of view through a wide-angle endoscope is superior to what a surgical microscope sees through a narrow nasal speculum, making it safer and more complete.
Dr. Sarang Gotecha performs transnasal endoscopic surgery at Manipal Hospital, Baner, Pune, in coordination with ENT surgical colleagues for the nasal component of the approach.
The pituitary gland - roughly the size of a pea - is called the 'master gland' because it controls the hormone output of most other endocrine glands: thyroid, adrenal glands, gonads and more. It sits just below the optic chiasm, where the nerve fibres carrying vision from both eyes cross.
Pituitary tumors (adenomas) arise from the cells of the pituitary gland. They are among the most common intracranial tumors, with autopsy studies suggesting that up to 25% of the general population have small pituitary adenomas - most never causing symptoms.
• Pressing on the optic chiasm → visual field loss (classically, bitemporal hemianopia - loss of peripheral vision on both sides)
• Compressing normal pituitary tissue → hormonal deficiency (hypopituitarism)
• Excess GH production → acromegaly (abnormal growth of hands, feet, facial features)
• Excess ACTH production → Cushing's disease (weight gain, hypertension, diabetes, mood changes)
• Excess prolactin → galactorrhoea (milk production outside pregnancy), infertility, menstrual irregularity
Surgery is recommended when vision is affected or the tumor is large with significant compression of normal pituitary tissue.
Non-functioning adenomas do not produce hormones in excess. They typically come to attention because of visual field loss (chiasmal compression) or as incidental findings on MRI. Surgery is recommended when vision is affected or the tumor is large with significant compression of normal pituitary tissue.
After surgery, visual field improvement begins within days to weeks in most patients, as the chiasm is decompressed.
Functioning adenomas require endocrine collaboration. In acromegaly (GH excess) and Cushing's disease (ACTH excess), surgery is the first-line treatment - removing the adenoma normalises or significantly reduces excess hormone levels. For prolactinomas, medical treatment (dopamine agonists) is usually first-line; surgery is reserved for drug-resistant cases or those with visual compromise.
Biochemical remission rates after endoscopic surgery for microadenomas (small tumors < 10 mm) can reach 85–90% in experienced hands. For macroadenomas with cavernous sinus invasion, complete remission is less predictable and combination with medical therapy or radiosurgery may be needed.
Craniopharyngiomas are benign but locally aggressive tumors arising from embryonic remnants near the pituitary stalk. They cause vision loss, growth failure in children and hormonal deficiencies. The extended endonasal endoscopic approach provides excellent access to infradiaphragmatic craniopharyngiomas, avoiding the need for a more complex craniotomy in selected cases.
The extended endonasal endoscopic approach can be extended beyond the pituitary to access the clivus - the sloped bone just behind the pituitary, in front of the brainstem. Clival chordomas and some clival meningiomas can be approached via this route, avoiding a larger skull base craniotomy.
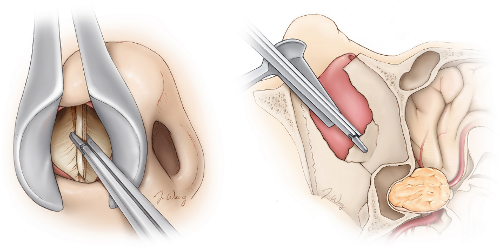
The operation is performed under general anaesthesia. The patient's nasal passages are prepared. The ENT surgeon creates the nasal corridor - widening the nasal passages and entering the sphenoid sinus - while the neurosurgeon guides the approach with the endoscope.
Once the posterior wall of the sphenoid sinus is opened, the floor of the sella turcica (the bony housing of the pituitary) is identified and opened. The tumor is removed using specially designed long angled instruments - curettes, suctions, ring curettes - while the surgeon watches on a high-definition monitor.
After tumor removal, the surgical defect is sealed - typically with fat graft, fibrin glue and sometimes a nasal septal flap - to prevent CSF leak (leakage of brain fluid through the nose), the primary complication to be avoided.
The procedure typically takes 2–4 hours for standard pituitary macroadenomas. There are no external incisions and no visible sutures.

• MRI pituitary (dedicated, thin-slice protocol) and CT base of skull for surgical planning
• Full endocrine workup (hormone levels, dynamic testing if needed)
• Ophthalmology review for visual field testing
After Surgery:• ICU or high-dependency unit: 1 night
• Hospital ward: 2–3 additional days
• Nasal packing (if used): removed before discharge
• Head elevation advised for 2 weeks to reduce CSF leak risk
• Nasal saline irrigation to keep passages clear
• MRI at 3 months to assess residual tumor and surgical cavity
• Endocrine review at 6 weeks and 3 months post-operatively
Most patients return to desk work within 2–3 weeks. Strenuous activity, nose blowing and sneezing are restricted for 4–6 weeks.
The wide-angle endoscope sees around corners - allowing visualisation of tumor extending laterally toward the cavernous sinuses, which the straight-ahead surgical microscope cannot see as well.
Better illumination:Light at the tip of the endoscope illuminates the surgical field evenly, eliminating the shadowing inherent in external light sources used with microscopes.
No nasal speculum retraction:The traditional microscopic approach required a rigid nasal speculum, causing pressure on the nasal septum and higher rates of nasal complications. Endoscopy avoids this.
Less post-operative nasal morbidity:Reduced nasal crusting, improved nasal airflow and less discomfort compared to the older approach.
