
Spinal trauma and fracture fixation in Pune is managed by Dr. Sarang Gotecha at Manipal Hospital, Baner. He treats cervical, thoracic and lumbar fractures using percutaneous pedicle screw fixation and open decompression-fixation, addressing spinal cord compression, instability and vertebral body collapse after road accidents and falls.
Lead with data: Spinal cord injury (SCI) affects over 15,000 new patients in India annually, with road traffic accidents responsible for 60–70% of cases. The tragedy is that a significant proportion of spinal cord injuries are either caused or worsened by inappropriate handling and delayed surgical treatment in the first hours after injury. Use this to underline the critical importance of rapid, expert assessment and timely fixation.
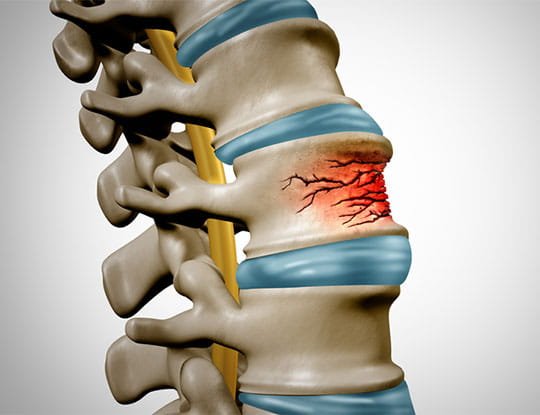
The spinal cord is the main highway of the nervous system - carrying every signal between the brain and the body. When the spine fractures - from a road accident, a fall, or a collision - the fragments of bone can compress or sever this cord. The result, if untreated, can be permanent paralysis.
Not every spinal fracture causes immediate cord injury. Many patients arrive with a fractured vertebra but intact neurological function - and the goal of treatment in these cases is to ensure that cord injury does not develop due to continued instability or delayed collapse.

Dr. Sarang Gotecha manages spinal trauma cases at Manipal Hospital, Baner, Pune. His expertise in both conventional open fixation and minimally invasive percutaneous approaches allows him to tailor the surgical method to the patient's injury pattern and overall medical condition.
A stable fracture is one where the spine's integrity is maintained sufficiently that no surgical intervention is needed - the fracture is unlikely to displace further and threaten the cord. A simple compression fracture of the vertebral body in an otherwise intact spinal column may be managed with a brace and physiotherapy.
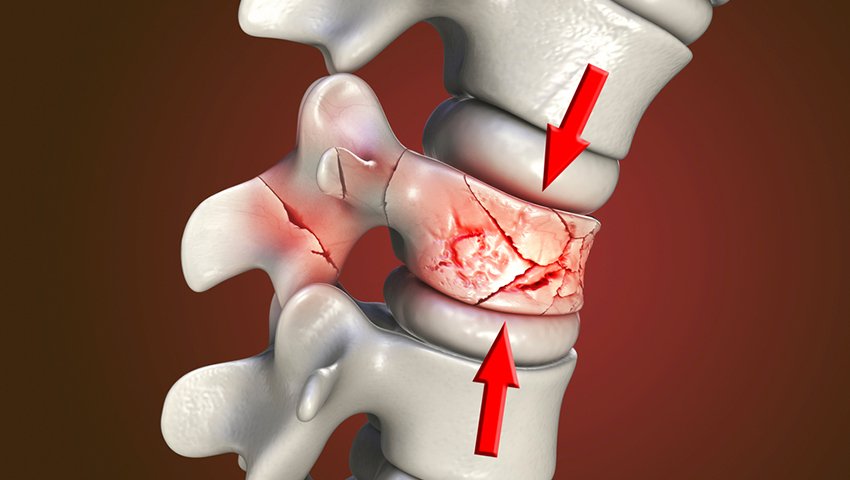
An unstable fracture is one where there is risk of further displacement, causing cord compression. Burst fractures (where bone fragments scatter into the spinal canal), fracture-dislocations (where the vertebral relationship is disrupted) and flexion-distraction injuries (seat-belt injuries) are typically unstable and require surgical fixation.
The most important distinction in spinal trauma is whether neurological function is preserved. A patient who walks into the emergency department despite having a cervical fracture - or one whose imaging shows severe canal compromise but who is neurologically intact - requires urgent surgery to prevent deficit. Delay is not acceptable.
A patient with an already-established complete spinal cord injury (no motor or sensory function below the injury level) may not recover function regardless of surgery timing. Surgery in these cases still serves to stabilise the spine and allow earlier mobilisation and rehabilitation.
Cervical fractures are the most dangerous spinal injuries because the cervical spinal cord, when damaged at high levels (C3–C5), can impair breathing. High-energy cervical injuries from road accidents or diving accidents require urgent evaluation and often surgical fixation - either from the front (anterior cervical discectomy and fusion, corpectomy) or from behind (posterior lateral mass or pedicle screw fixation).
Cervical fractures that compress the cord in a neurologically deteriorating patient are surgical emergencies at Manipal Hospital, Baner.
The thoracic spine is relatively protected by the rib cage, so fractures here typically require significant force - high-speed road accidents, falls from height. Burst fractures with retropulsed bone into the thoracic canal and neurological deficit require posterior decompression and fixation , sometimes with anterior reconstruction if the vertebral body is completely destroyed.
Lumbar fractures - particularly burst fractures at L1–L2 (the thoracolumbar junction, the most common fracture level) - are common in falls from height and road accidents. These injuries may cause cauda equina syndrome (compression of the nerve roots below the spinal cord) with bladder, bowel and leg weakness - a surgical emergency requiring urgent decompression and fixation.

Standard posterior approach for spinal fracture fixation involves a midline incision, muscle dissection, pedicle screw placement above and below the fracture level and rod fixation to restore alignment. When the spinal canal is compromised, laminectomy removes the bone pressing on the cord. This approach is comprehensive and allows full decompression and reconstruction.
For fractures that require stabilisation but not decompression (stable burst fractures with no neurological deficit, for example), percutaneous pedicle screw fixation achieves fixation without open muscle dissection. Two to four small stab incisions allow screw insertion under fluoroscopic guidance. Recovery is significantly faster than open fixation, with less blood loss and shorter hospitalisation.
Dr. Gotecha's MISS training in Seoul makes him one of the few spine surgeons in Pune with fellowship-level proficiency in percutaneous fixation for trauma.
When a vertebral body is destroyed beyond the capacity of posterior instrumentation to reconstruct (typically at the cervical or thoracolumbar spine), an anterior approach is used to remove the destroyed bone, restore height with a cage or strut graft and fix with an anterior plate. This is sometimes combined with posterior fixation in a staged or single-sitting procedure.
Emergency decompression - surgical relief of cord compression in a patient with progressive neurological deficit - is one of the time-sensitive interventions in neurosurgery. Animal studies and clinical evidence suggest that earlier decompression (within 24 hours of injury) leads to better neurological recovery. The STASCIS study demonstrated a 2-grade improvement in ASIA motor scores for patients decompressed within 24 hours versus later.
At Manipal Hospital, Baner, the pathway from emergency presentation to surgical decompression is as short as clinically possible - CT and MRI within the first hour, anaesthetic assessment in parallel and surgical fixation without delay when indicated.
• Stable fractures managed in a brace: Usually heal well over 8–12 weeks. Follow-up imaging confirms healing. Risk of delayed instability is low with appropriate immobilisation.
• Unstable fractures managed without surgery: Progressive deformity, delayed kyphosis and late-onset neurological deficit. This outcome is preventable with appropriate fixation at the right time.
• Cord-compressing fractures not decompressed: Ongoing cord injury and loss of neurological recovery potential. The window for effective decompression may close within 24–72 hours.
Dr. Gotecha's approach: surgery when stability or neurological protection requires it, conservative management when clinical evidence supports it. He does not recommend unnecessary fixation and he does not postpone necessary fixation.
