
Skull base surgery in Pune is performed by Dr. Sarang Gotecha at Manipal Hospital, Baner. He treats acoustic neuromas, petroclival meningiomas, chordomas and glomus tumors using advanced skull base approaches. These procedures protect cranial nerves and preserve function while achieving maximum tumor removal at Pune's most equipped neurosurgical facility.
Skull base tumors are rare enough that most neurosurgeons see only a handful per year. Yet in a city of 7 million like Pune, several hundred patients per year are diagnosed with these conditions - and many are told to go to Mumbai or Delhi for surgery. Use this to position Dr. Gotecha's specialist training as filling a genuine gap in Pune's surgical landscape, enabling patients to receive world-class skull base care close to home.
The skull base is the floor of the skull - the bony platform on which the brain rests, perforated by foramina (openings) through which blood vessels and all 12 cranial nerves exit. It is one of the most anatomically crowded regions of the human body and tumors that arise here press against structures that control hearing, facial expression, swallowing, eye movement and voice.
Operating at the skull base requires a different level of surgical planning and execution than most other neurosurgical procedures. The routes to reach these tumors are narrow, the adjacent nerves are fragile and the blood vessels are large and critical. Getting it right demands experience, appropriate tools and - very often - a team approach with ENT surgeons and neuro-anaesthetists.
Dr. Sarang Gotecha performs skull base surgery at Manipal Hospital, Baner, Pune. His training at international centres included skull base surgery techniques and he applies them to cases that previously required referral out of Pune.

The skull base can be divided into three compartments - the anterior (front), middle and posterior fossa - each housing different brain structures and cranial nerves. Tumors in each compartment require different surgical approaches:
• Anterior skull base: Frontal lobes, olfactory nerves, optic nerves. Approached via subfrontal or endonasal (through-the-nose) routes.
• Middle skull base: Temporal lobes, trigeminal nerve (V), abducens nerve (VI). Approached via middle fossa or transpetrosal routes.
• Posterior skull base: Cerebellum, brainstem, cranial nerves VII-XII. Approached via retrosigmoid, far-lateral, or translabyrinthine routes.
The most common posterior skull base tumor, acoustic neuroma arises from the sheath of the vestibular (balance) nerve in the internal auditory canal. As it grows, it compresses the facial nerve (causing facial weakness), cochlear nerve (causing hearing loss) and eventually the brainstem. Surgical removal aims to preserve facial nerve function - measured by the House-Brackmann scale - while fully removing the tumor.
Hearing preservation is attempted in selected cases using a retrosigmoid approach when residual hearing is worth preserving pre-operatively.

These meningiomas arise in one of the most surgically challenging locations - the clival surface adjacent to the brainstem, surrounded by multiple cranial nerves and the basilar artery. Complete surgical removal carries significant risk. Dr. Gotecha approaches these with careful pre-operative planning, intraoperative neurophysiological monitoring and the goal of maximum safe resection rather than completeness at any cost.
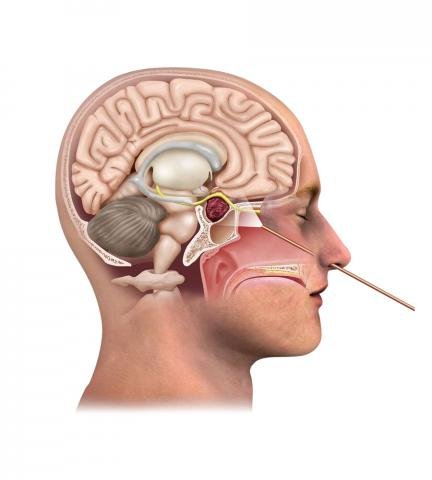
Chordomas are rare, locally aggressive tumors that arise from remnants of the embryonic notochord - most commonly at the clivus (skull base) or sacrum (spine). They are not malignant in the traditional sense but grow destructively and recur after incomplete resection. Extended endonasal endoscopic approaches or open skull base approaches are used depending on the tumor's location and extent.
Glomus tumors of the skull base (glomus jugulare, glomus tympanicum) arise from paraganglionic tissue near the jugular foramen. They are highly vascular and encase multiple lower cranial nerves (IX, X, XI). Surgical management requires pre-operative embolisation to reduce blood loss, followed by careful microsurgical resection.

There is no 'one approach fits all' in skull base surgery. The route to a tumor depends on its location, size, vascularity, relationship to cranial nerves and whether the goal is complete removal or subtotal resection with adjuvant radiosurgery.
Common approaches used by Dr. Gotecha include:• Retrosigmoid craniotomy - for posterior fossa tumors including acoustic neuromas
• Subfrontal craniotomy - for anterior skull base lesions
• Orbitozygomatic approach - for middle fossa, cavernous sinus and parasellar tumors
• Far-lateral approach - for foramen magnum and lower clival lesions
• Extended endonasal endoscopic approach - for clival chordomas and selected anterior skull base lesions, coordinated with ENT colleagues
In skull base surgery, the most feared complication is not the tumor itself but the nerve it has grown around. Facial nerve weakness after acoustic neuroma surgery, lower cranial nerve palsies after glomus jugulare surgery and abducens nerve palsy after petroclival meningioma surgery can significantly affect quality of life.
Dr. Gotecha uses intraoperative neurophysiological monitoring (IONM) during skull base procedures - continuous monitoring of cranial nerve function throughout the operation. When the facial nerve is at risk, free-running EMG monitoring provides real-time feedback that alerts the surgeon to proximity of the nerve before any injury occurs.
This monitoring is not available at all neurosurgical centres in Pune. At Manipal Hospital, Baner, it is routinely available for complex skull base cases.
A general neurosurgeon who performs 2–3 skull base cases per year has fundamentally different outcomes from a specialist who has received dedicated training at high-volume centres. The anatomy at the skull base is three-dimensional in a way that textbooks cannot fully convey - it requires hands-on training under expert guidance.
Dr. Gotecha's exposure to skull base surgery at the National Neuroscience Institute, Singapore, provided this high-volume training environment. NNI is among Asia's busiest neuroscience centres and the skull base volume there is significantly higher than what is seen in most individual hospitals in India.
